Prototype device effectively treated multiorgan failure
A newly published study describes how, in a small pilot, patients were rescued from their bodies’ cascade of deteriorating function.Media Contact: Brian Donohue - 206-543-7856, bdonohue@uw.edu
Clinical trial results published last week describe a novel medical device that, in a 10-patient pilot, showed remarkable success at rescuing people from multiorgan failure caused by acute-on-chronic liver failure.
All 10 patients had been officially listed for liver transplant but were delisted when their clinical condition deteriorated considerably amid multiorgan failure. They all underwent treatment on the new device and became healthy enough to discontinue supportive measures and be relisted for transplant.
Half ultimately received a lifesaving liver graft or spontaneously recovered (one patient), while the other five died due to the lack of available donor organs.

The findings appear in the Journal of American Society for Artificial Internal Organs. The co-lead authors from the University of Washington are Dr. Suhail Ahmad, a nephrologist and professor emeritus in the UW School of Medicine, and Dayong Gao, a professor in the Department of Mechanical Engineering. They also are the device’s lead developers.
Although acute-on-chronic liver failure was the inciting factor for patients in the trial, multiorgan failure (MOF) is a familiar condition in major metro hospital ICUs.
“For a long time, multiorgan failure was thought to be associated with sepsis only, but now we know that patients who have burn or trauma or severe damage to one vital organ sometimes can start this cascading failure of multiple organ systems,” said Ahmad.
“Various clinical conditions are severe, either at presentation or they become severe within the course of hospitalization. Sepsis, severe pulmonary and cardiac injury, advanced liver and kidney failure, severe trauma and burn: All of these can lead to other organs becoming involved, often in a cascading fashion,” he said.
MOF is as close to death that anyone can be and still recover, Ahmad suggested. He identified devices that support individual organs: ventilators to assist lungs, hemodialysis to filter toxins normally cleared by kidneys, and heart-lung bypass to send oxygenated blood to the body while those two organs rebound from acute injury or chronic illness.
These instruments, deployed in tandem with medications, often enable patients to survive and leave hospitals on their feet.
Hospital statistics on MOF vary among studies. In-hospital mortality is much higher in patients who have MOF (65%) compared with those without organ failure (6%), according to a 2011 paper. MOF is responsible for 50-60% of all trauma deaths, 30% of all burn deaths and 50% of all pancreatitis deaths. Another paper reported that patients with liver failure who develop MOF are particularly at higher risk of death: 45%, 65% and 90% mortality with one-, two- or three-organ failure, respectively.

Two common traits of multiorgan failure, however, can thwart doctors’ best efforts to keep organs viable: Toxins accumulate as a result of liver failure and fluids increase in tissues throughout the body. These complications undermine the function of all vital organs, especially the heart, lungs and brain, and can be challenging to resolve.
“My expertise is in removal of toxins which build up as a result of kidney failure,” said Ahmad, a practitioner of 50-plus years who trained under kidney-dialysis pioneer Dr. Belding Scribner. “I wanted to understand: How can we remove the liver toxins, which are not removed by kidney dialysis, and save these patients? My thought was to take the dialysis machine and attach another instrument off the shelf and convert it to a liver-kidney dual support.”
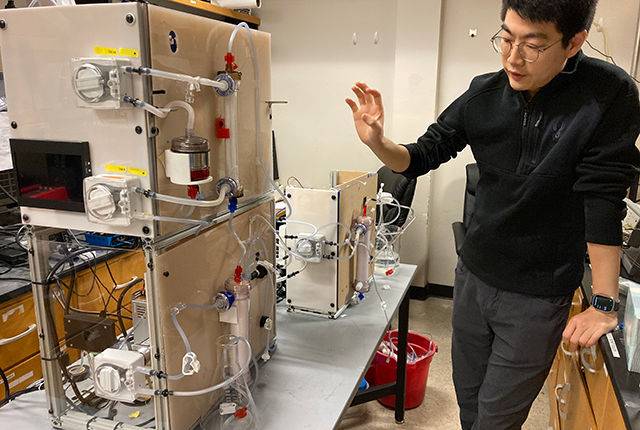
Around 2008, Ahmad and Gao, from mechanical engineering, started developing what has become the Artificial Multi-organ Replacement System (AMOR). They focused on the device’s capacity to clear toxins in the blood that accumulate with liver failure.
And they wanted to improve on an existing liver-detoxification device used by U.S. hospitals, the Molecular Adsorbent Recirculating System (MARS).
"One of the very exciting features of the AMOR system is that it can remove a large volume of life-threatening excess body fluid in a way that cannot be matched by any other currently-used artificial organs, such as the artificial kidney," said co-senior author Gao.
The AMOR technology, he said, flexes to each patient’s circumstances.
"The machines currently used in hospitals can treat only one organ failure at a time, but AMOR combines multiple organs' functions all together. Depending on a patient's needs, AMOR can be used to replace one, two or more organ functions, including kidney, liver, lungs or heart. We hope to further improve the AMOR design to make it more convenient to use not only at hospitals and ICUs, but also rural clinics and at home," Gao said.
The clinical trial emerged after Ahmad was approached by the liver-care team.
“In (acute-on-chronic liver failure) patients who are on the transplant list, their organs start failing and they end up in the ICU, removed from the transplant list. Kidney dialysis alone doesn't seem to help, so these patients also are on ventilator, on blood-pressure support. So multiple external support,” he said.
“In the trial, bilirubin removal with our machine was quite good. What surprised me was that these patients had been on various dialysis treatments that could not remove fluid effectively. But on our machine, they were losing liters of fluid in one treatment. I was surprised and amazed at this result — which helped the lung and heart function.
“Our machine, the way we designed it, I think removes toxin more efficiently. But the biggest difference was that MARS only removes liver toxins, but our machine is connected to a (kidney) dialysis machine, so was able to significantly remove fluid and kidney toxins and other toxins at the same time. The combined effect appears to be a lot better than what is published on MARS.”
The device’s next step, Ahmad said, would be a larger trial to prove its efficacy. “If our system works, and I think it will, then we can make it available to all ICU patients, no matter what the disease is. You remove the excess body fluid and toxins, thus improving their outcome.”
Related: A healthy collaboration (Mechanical Engineering feature story)
For details about UW Medicine, please see our About page.