Radiology embraces automation to meet clinical headwinds
A vision to streamline the admin side of patient care helps UW maintain its role as a research powerhouse in the field.Media Contact: Brian Donohue - 206-457-9182, bdonohue@uw.edu

Need an MRI or some other medical scan? Your wait seems destined to grow, at least in the near term.
The aging U.S. population is ratcheting up demand for medical images. In parallel, the workforce of radiologists and technologists is shrinking — from retirements, hospital consolidations and other industry dynamics. The depleted staffs that remain face higher patient expectations for communication, perhaps as a result of recent access to telemedicine and electronic medical records.
These clinical headwinds are amplified in academic radiology departments. Some are deciding that meeting this greater clinical demand means shuttering decades-old research programs that have contributed to the effectiveness and safety of disease-illuminating technologies.
“In the U.S., there are around 250 academic radiology departments. Everybody’s in the same squeeze,” said Paul Kinahan, vice chair for research and professor of radiology at the University of Washington School of Medicine. “Probably a couple of dozen are our peers in terms of grant funding and innovating with research. But that number could shrink to 10 or 12 in the next few years.”
Kinahan and his department chair, Dr. Dushyant Sahani, recently described these converging forces as unsustainable.
“Right now, we face escalating demand for imaging and image-guided procedures. Patient cases are more complex, and we are being asked to do more, too. It’s no longer just do a scan and write a report,” Sahani said. “If we don’t innovate, we’ll either burn out or have to deny people care.”
His vision to bring the department forward, with both clinical care and research, requires the creation of “a seamless digital journey for our patients.”
At every juncture of the patient-care experience, UW Medicine Radiology will explore commercial technologies to automate patients’ experience of care, Sahani said. Such a pivot will necessitate working more closely with technology manufacturers whose software and services might help meet the changing priorities of patient care.
“Imaging is moving from (radiologists’) predominantly qualitative and visual assessment to quantitation of the digital data,” he said. “There is evidence that, by extracting detailed data from CT images, radiologists might be able to predict patients’ risk of future events and chronic conditions.”
He referred to GE Healthcare, a vendor and research partner with the department for 30 years. A new collaboration with the company prioritizes care pathways for which GE’s technologies are already in-house, including CT, molecular imaging and theranostics, an emerging area that combines targeted imaging and therapies to see and destroy cancer cells.
“There are AI tools that GE has developed and we’re trying to see if incorporating them will help us extract digital information from the scans like: What is the organ volume? How much is the muscle mass? What is visceral fat? What is the total burden of a disease in patients with cancer? Currently we provide these services in limited capacity,” Sahani said.
In parallel, other companies’ technologies are being evaluated to address the department’s growing burden on the administrative side of patient care.
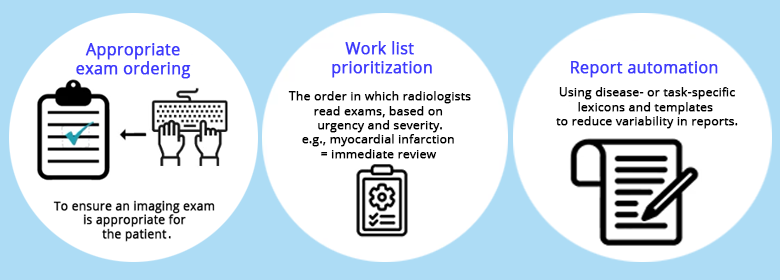
Sahani showed an illustration of his team’s responsibilities tied to a single patient referral for CT scan. It highlighted several discrete tasks that pose opportunities for automation: appointment-scheduling, choosing patient-specific imaging protocols, prioritizing work, distributing scans to appropriate reviewers and caregivers, communicating results to patients, and others.
Collaborations to promote efficiencies in these areas are under consideration or in the works with other firms. For instance, Nuance, a Microsoft-owned company, has AI-guided transcription and report-generation software. Aidoc develops computer-aided triage and notification systems.
By deeply exploring automation’s advantages on the clinical side, UW Medicine radiologists can, perhaps paradoxically, keep a firm footing in the research that drives their field forward, Kinahan suggested.
“Patients are first, but if we want to improve care, we have to continue to innovate. And for us to get any innovations into practice, we have to work with industry. Ideally, we influence their products for the benefit of future patients, whether or not we buy them,” he said.
With each collaboration, improvement happens for both parties, he said.
“New capabilities help us, and partners get our feedback about how their software or hardware might be more useful, even with some small change,” he said. “Our research reputation has made us a trusted source of feedback for products’ clinical value.
For details about UW Medicine, please see our About page.