Q&A: Mini organs offer hints to COVID-19’s kidney injury
Study: Blacks and Hispanics with Type 1 diabetes were three times more likely to be infected and twice as likely to die from the novel coronavirus.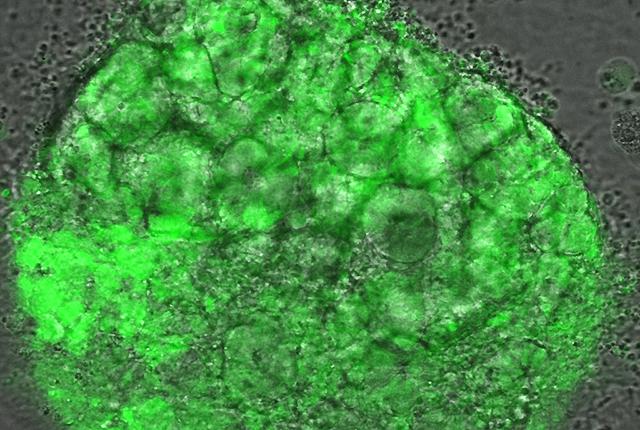
People hospitalized with COVID-19 can experience myriad symptoms. We’ve heard a lot about the virus’ ability to congest lungs, to fog the brain, to inhibit the senses of smell and taste, and to cause crushing fatigue. One of COVID-19’s lesser-reported injuries involves kidneys.
Dr. Benjamin “Beno” Freedman, a UW Medicine nephrology researcher, has been studying these injuries since last summer. He’s using organoids, complex mini-organ structures grown from stem cells, which model kidney function and can be closely monitored for changes at a cellular level.
He discussed the research in this Q&A, which has been edited for clarity.

Q. Are COVID-19-related kidney infections easily detected – or are injuries pretty advanced by the time they are recognized? How does that emergence affect patient-treatment decisions?
A. Among hospitalized patients with COVID-19, many experience acute kidney injury – more than 25%, according to some reports. This is really the kidneys’ equivalent of a heart attack. Basically they rapidly stop functioning.
Doctors can detect these problems in clinic; they can see that a patient’s kidneys are not functioning properly. But it’s hard to know exactly why. By the time you get samples of a patient’s kidney tissue, the disease often has progressed to a late stage, so you don’t know whether the kidney cells were damaged directly or indirectly.
Many of the patients end up on dialysis to temporarily replace kidney function while hoping their own kidneys have a chance to recover.
Q. Dialysis is a last-resort type of measure, isn’t it?
A. Yes. Dialysis can save someone’s life but it does not heal their kidneys. What we need is a fast-acting treatment that can help heal the injury. But to identify an effective treatment, we first need to understand the specific causes and mechanisms of COVID-19-related kidney dysfunction.
We also don’t know why certain patients are more vulnerable. It's not like you can easily get a sample of kidney tissue to suss that out.
Q. This is where the organoid system comes into play?
A. Yes, because you have a little piece of human kidney structure. It looks and functions similar to kidney tissue at a rudimentary level. We can perform careful experiments to see exactly what's happening; you can watch these kidney cells under the microscope and begin to understand what is occurring in the context of COVID-19. We are using organoids as a surrogate for people.
Q. What specifically do you hope to learn from the organoids?
A. We want to establish the mechanisms of injury. It could be a direct infection of certain cells in the kidney or an indirect effect of a body being in an inflammatory state because of a raging virus. That's what we've been trying to figure out.
Now we have an idea of what’s going on and we’re beginning to test different types of treatments against those infections to see whether they can be helpful in either preventing the injury in the first place or treating it afterward. We’re starting with therapies that are already established, identified as likely to help, and moving toward therapies whose value is less known.
Q. Are you working with one strain of COVID-19 or multiple strains?
A. The COVID-19 being tested is all the same strain. It is being cultured in the BSL-3 lab of UW Medicine immunologist Michael Gale.
Q. Can you give a hint about the findings you’ll report?
A. One thing we found is that the organoids can be infected; infectious virus can get into cells in kidney organoid cultures and is capable of replicating under those conditions. Others have begun to report this in literature as well. And we can shed some light on which types of kidney cells appear most susceptible to COVID-19.
We're putting a manuscript together that we’ll aim to submit in the next few months.
– Brian Donohue, 206.543.7856, bdonohue@uw.edu
For details about UW Medicine, please see our About page.