Q&A: If you’re just finding out you have dense breasts
An FDA mandate means that millions more U.S. women will get their first such notice this year. A mammography expert offers context.Media Contact: Brian Donohue - 206-543-7856, bdonohue@uw.edu

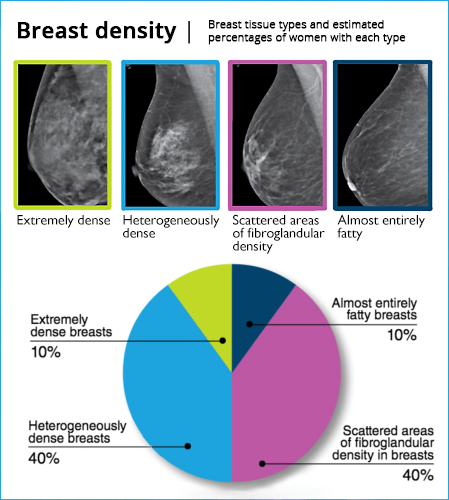
About half of all women over age 40 have breasts that can be clinically characterized as “dense.” It’s a term that has begged for more context since radiologists, more than 25 years ago, realized that breast tissue could be very fatty or very fibrous or somewhere in between. They subsequently discerned that fibrous breasts are associated with more cancer risk.
Last September, the Food and Drug Administration mandated that all U.S. women should be formally notified of their breast tissue composition after getting a mammogram. (This decision followed laws already on the books in 39 states to provide women the same information.) But the notification comes with no clarity or reassurance about cancer risk and no suggestion of what a woman should do, or expect, if she’s learning for the first time that her breast tissue is dense.
Dr. Christoph Lee, a UW Medicine radiologist and mammography expert, coauthored an article published this week in JAMA. The piece, Lee said, aims to give key information to clinicians “who are not used to being bombarded with questions about breast density” and who will need to have shared decision-making conversations with patients.
Below, Lee discusses the article, cowritten with Dr. Joann Elmore of UCLA, and addresses other questions relevant to women who undergo breast mammography. This Q&A was edited for clarity and length.
Q: What do these FDA-mandated notifications tell women?
Lee: After a mammogram, women are told directly whether they have dense or non-dense breasts, and that they may benefit from speaking to their primary-care provider about potential supplemental screening if they have dense breasts.
For context, of the 40 million women who get mammograms ever year, about 20 million are going to be told that they have dense breasts.
Q: Do you think this brief notice helps recipients, or might raise alarm?
Lee: I think both. From a patient-advocacy perspective, the goal was to have more women informed and aware that breast density is a risk factor for developing breast cancer, and for having breast cancer missed on a mammogram. But it also causes unnecessary alarm because breast density is a moderate risk factor, and just one of many risk factors.
Q: How do you describe the cancer risk of dense breast tissue?
Lee: It confers a very small amount of absolute increased risk. For instance, for a woman in her 40s, the risk from dense breasts alone is comparable to having an aunt or cousin who had breast cancer sometime in their life. That type of family history is extremely common, and it doesn't bump a woman from average risk to high risk.
To be categorized as having higher risk, a woman would need to have other factors such as a history of breast biopsy or primary relatives like a mother or sister with breast-cancer history, or a known genetic mutation.
Q: Based solely on being notified of having dense breasts, should a woman proactively seek out screening technologies that are more sensitive than a mammogram?
Lee: No. Just because a woman has dense breasts and a small, incremental bump in their absolute risk doesn't put them in a category that requires anything beyond a usual mammogram — a routine 2D or 3D mammogram every one to two years starting at age 40.
A 3D mammogram, or digital breast tomosynthesis, is now the preferred modality for breast cancer screening, and prevalent throughout the country: 75% of all mammography units used in the U.S. are 3D-capable.
Overall, the ability for a mammogram to detect the presence of cancer is about 88%. If, based on a mammography screening, a radiologist notes that a patient is among the 10% of women whose breasts are not just “heterogeneously dense” but “extremely dense,” that ability to detect cancer drops to about 75%.
Q: At what point does it make sense for a woman to pursue a more sensitive screening technology?

Lee: Findings that specify the degree of breast density are entered into the patient’s medical record. So an individual who has extremely dense breasts can talk with their gynecologist or primary-care provider about getting a formal risk assessment.
Density is one of the risk factors that's incorporated into the prediction, but it also includes things like family history, breast biopsy, age. All of that is input to a risk-prediction tool to come up with a five-year, 10-year and lifetime breast cancer risk score. Based on that score, we can determine whether supplement screening is required.
For women whose lifetime risk is greater than 20% according to a formal risk calculator, we recommend breast MRI in addition to their routine mammogram. Breast MRI actually has the highest sensitivity; it detects more than 90% of cancers that are present. But the problem with MRI is that it's so sensitive that there are a lot of areas that may appear like cancer but that are normal. Thus, women tend to get a lot of false positives and unnecessary breast biopsies with this modality. So we tend to reserve breast MRI for women whose risk for developing breast cancer is known to be higher.
This conversation should cover an individual woman's values regarding the benefits of early cancer detection versus the risks of false positives, because the risk of false positives is very real. The more you look, the more you're going to find — and the majority of the things we find are benign and not cancer.
Q: Your paper mentioned that the FDA’s directive was not based on scientific study, but on decades of grassroot advocacy from patient groups. Don't we want these mandates to be based on evidence?
Lee: Yes, but I think a lot of what happens with FDA regulations relies on stakeholders speaking up. And not all guidelines and recommendations are purely evidence-based. The patient-advocacy groups did an amazing job of telling personal stories and making their voices heard about a cause that they cared deeply about. I think their intentions were always good: having women more informed about their breast-density status and breast-cancer risk.
Photo credit: The breast scan image, published by Leah Small, was republished under Creative Commons License 2.0.
For details about UW Medicine, please visit https://uwmedicine.org/about.