Lancet report goal: Halve premature mortality by 2050
Q&A: A UW Medicine coauthor gives context to data showing poor U.S. progress on the metric, relative to other nations’ rates.Media Contact: Brian Donohue - 206-543-7856, bdonohue@uw.edu

A report published this month in The Lancet focuses on a global concern: premature death. It argues, optimistically, that countries can cut their populations’ risk of premature death in half by 2050, if they choose.
Dr. David Watkins is an associate professor of medicine and global health at the University of Washington School of Medicine and a hospitalist at Harborview Medical Center. He serves on The Lancet Commission on Investing in Health, which produced the report “Global health 2050: the path to halving premature death by mid-century.” Watkins discussed the findings via email.

Q: What’s the context for the report?
Watkins: The commission was formed in 2012. It brought together health experts and economists to make the case to governments to put more money into high-value healthcare. (Previous reports can be found here.) I think we’ve made a major impact on international health policies. Our work has been taken up by politicians, development aid agencies, and influential people around the world.
Since 2022, though, pandemic burnout, inflation, misinformation and other factors have led many governments to cut healthcare funding. In early 2023, the Lancet’s editor-in-chief asked us to prepare a new report that provides a vision and goal for public health. Our main message is that countries can reduce their populations’ risk of premature death by 50% by 2050, compared to 2019. We call this goal “50 by 50.” Our research concluded that this goal is feasible for countries both rich and poor.
Q: How did your team define ‘premature’ death?
Watkins: Any death under age 70. The late epidemiologist Richard Doll once wrote, “In old age death is inevitable, but death before old age is not.” Deaths before 70 have a big psychological and economic impact on families and caregivers. We found that just 15 health conditions account for most of the avoidable death under 70. Focusing health spending on these conditions could help countries achieve the 50 by 50 goal. The report also discusses how health systems and financing must change to meet the goal. I led that part of the report.
Q: What are a couple of points from the report that you’d want a layperson to focus on?
Watkins: It’s a global report, but I think a few things stand out for a U.S. lay audience.
First, primary healthcare saves lives. Nearly all the interventions we recommend are simple things that any primary-care provider can do, yet they’re not being done as often as they should. Get your blood pressure checked regularly. If your age makes you eligible, get screened for common cancers. If you’re struggling with addiction, get help. And so on.
Second, we need healthcare reform. Compared with other rich countries, the U.S. is doing very poorly on our metric of death before 70. With elections nearing, push your politicians to take health seriously. There are a range of bipartisan policies that could reduce premature death.
Finally, we need to prepare for the next pandemic. Between now and 2035, there is a 1-in-4 chance of a pandemic like COVID-19 or worse. Between now and 2050, the chance is more like 50-50. Voice your support for public health authorities in the U.S., who need more funding to work with international partners to do better surveillance and to share data quickly, so we don’t repeat the mistakes of COVID-19.
Q: What are major causes of premature death in the United States?
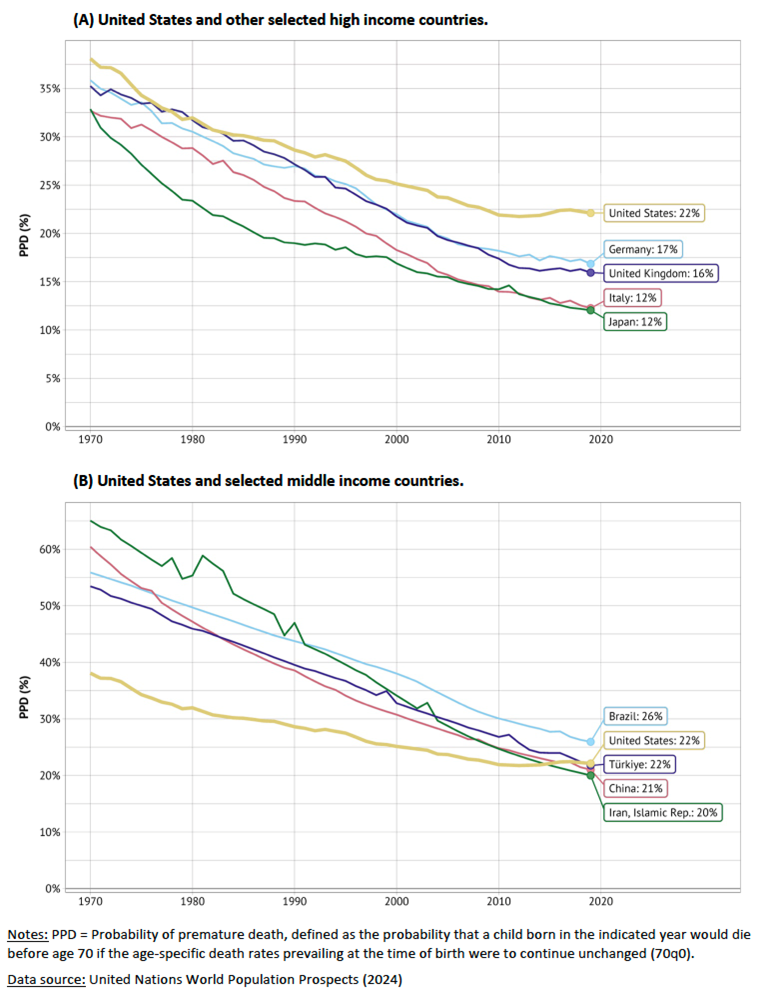
Watkins: Mostly heart disease, cancer, and injuries (including suicide). Our report shows that the U.S. is making very slow progress on reducing premature death, especially since 2010. In fact, the U.S. looks more like Iran or China than the UK or Japan when judged by premature death rates. (See graphic at bottom of this page.)
Q: Can you relate the findings to your clinical care at Harborview Medical Center?
Watkins: We see a lot of avoidable death among middle-aged adults, including those struggling with housing insecurity. A concrete example is death from opioid overdose, which we see all the time at Harborview. Contrast this with a country like Norway, where access to addiction treatment is excellent, homelessness is low, and overdose deaths are one-fifth of what they are in America. The social and economic despair here is abnormal for a rich country.
Q: From your point of view, are there paths to reducing premature death that look relatively easier to achieve, and paths that look like stretch goals?
Watkins: Yes. The blood pressure and cancer screening examples I mentioned previously apply here, too. We know these interventions work, but we just need to implement them better. Some pathways are harder, though. For example, we don’t have as many effective interventions for obesity. Some countries are starting to tax junk food and use the money to make fruits and vegetables more affordable. We can learn from these experiences.
The main message of our report is that 50 by 50 is a prize within reach for all countries, even the U.S. But politicians must choose to make health a priority. If they do not, their citizens should hold them to account.
For details about UW Medicine, please visit https://uwmedicine.org/about.