Could a pacemaker draw energy from the heart itself?
Q&A: Physician-scientist Babak Nazer explains why the wireless devices need better battery life, and his vision to make it happen.Media Contact: Brian Donohue - 206-543-7856, bdonohue@uw.edu

Dr. Babak Nazer is a UW Medicine physician-scientist specializing in heart rhythm disorders. Last month he presented a proof-of-concept research abstract that generated significant interest at the American Heart Association Scientific Sessions. It showed that a pacemaker, a device that helps a heart maintain a healthy beat, could be made with materials that enable it to partially recharge itself to extend its battery life.
I talked with him about the invention and the patients he hopes might one day benefit from such an advance. (This Q&A has been edited for clarity and length.)
Q: Which patient demographic gets most pacemakers?
Nazer: The most common risk factor is age, and most recipients are 60 and above. With our aging population, the incidence of new pacemakers is increasing. In parallel, the adult congenital heart disease population, based on improved surgical techniques earlier in life, is now living much longer and a lot of those early-life surgeries are creating a need for pacemakers in the 30 to 50-year-old age. So the prevalence of people who are living with a pacemaker is growing — and all those devices need battery changes over time.
Q: Let’s talk about the devices.
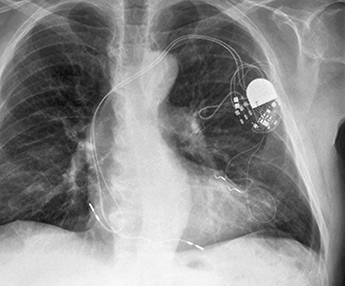
Transvenous pacemakers are the older, tried-and-true version. We make an incision under the left collarbone, and one, two or three wires, or leads, are navigated through a vein into separate locations in the heart. At the other end they are connected to a small generator that has a battery and circuitry. The generator sits just under the skin beneath the incision. It’s designed to be replaced every seven to 10 years, depending on the heart’s pacing needs.
That's fairly straightforward: Open the incision, replace the generator, reconnect the leads and close up. Patients usually tolerate the procedure well, but every time you open the pocket, it heightens the infection rate. The leads are in the bloodstream and if bacteria get into the blood, they can grab onto the wires and they cover themselves in what's called a biofilm. Antibiotics can't get to them, so the whole device almost always has to come out, which is much harder.
The leads also bend with every beat of the heart, and if a lead shows signs of impending failure, we put a new one in and either extract the old one, which can be risky, or leave it in the vein. Adding more leads can start to slow venous blood flow or create problems if the patient needs some other procedure.
Q: These issues motivated leadless pacemakers?
Nazer: Yes. The first human implant was in 2014 and it was intended to overcome those limitations. The device is about one-third the volume of a AAA battery. From an infection perspective, it's fabulous: Infections of leadless pacemakers are virtually unheard of. We enter through a vein in the groin and implant the pacemaker in the right ventricle. But we don’t leave anything in the veins, so barring an infection at the needle-hole site (at the groin), the bloodstream is protected.
Q: What about the battery in leadless devices? Changing them out would seem to be much more complicated.

Nazer: Batteries in leadless pacemakers are estimated to last between five and 12 years, again, depending on pacing. Some of these devices are marketed as retrievable, with the idea that electrophysiologists would swap out a patient’s pacemaker when the battery signals it needs replacing, but those claims are based on data suggesting about 90% of them could be retrieved after two years.
So we don’t know how retrievable they’re going to be after five, 10 or 12 years, because the longer the dwell time, the more endothelial tissue grows around the device and encapsulates it in the right ventricle. At the very least, getting these devices out will require an invasive procedure for patients, possibly with a high complication rate. The other option is to put a second device next to the first, but that can compromise safety or space in the right ventricle.
So I think there’s merit to developing technology that prolongs battery life to reduce the medical burden of multiple implants, and retrievals, and start expanding access of leadless devices to younger patients.
Q: Your team recently showed a pacemaker can create some of its own energy, thereby resulting in longer battery life. How did that project start and how’d you decide on what material to use?
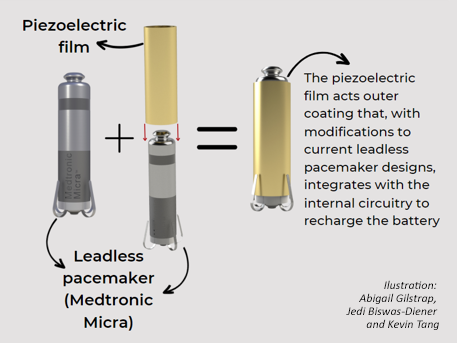
Nazer: My research collaborators and I work on ultrasound. Ultrasound transducers are made of piezoelectric materials, which convert energy bidirectionally. For ultrasound, we put voltage into them and get pressure out, as sound is really just oscillating pressure waves. With piezoelectric materials, I figured we should be able to turn the oscillating pressures of the right ventricle backward into voltage. In the lab, that’s what we saw: We developed a piezoelectric housing for a leadless pacemaker, and in a cardiac pressure simulator it generated a voltage. It raised the question of whether we could harvest any of that energy to extend battery life.
Q: With the prototype, did you have a goal amount or percentage of energy you wanted to harvest?
Nazer: We mainly wanted to prove the principle that it can be done without significantly enlarging the device or how it would be implanted.
I arbitrarily thought it’d be great to harvest 20% of the energy needed for a pacemaker’s next beat. That’s still a long-term goal. Ultimately it will be up to the pacemaker manufacturers, the patients and all the providers how much energy-harvesting they want to see before helping us translate this idea into a clinically viable product.
Q: Your device achieved a 10% energy recapture. Do you think that’s clinically meaningful?
Nazer: Not yet, and that’s why I’m humble about this project. I also point out that pacemakers have other functions beyond just powering the next heartbeat. But our prototype represents only six months of work of three graduate students working with my lab and the UW Bioengineering’s Master of Applied Bioengineering program. So, I’m very proud of what we achieved in that little time, and we have ideas and resources for improving that efficiency.
(Nazer credits engineers Abigail Gilstrap, Jedi Biswas-Diener and Kevin Tang, as well as Mohammad Malakooti in the Department of Mechanical Engineering, as the prototype’s major contributors.)
For details about UW Medicine, please see our About page.