Clinicians quickly grew adept at ID’ing mpox, study shows
The ability to accurately make a quick, provisional diagnosis may help infected patients get treatment sooner.Media Contact: Brian Donohue - 206-543-7856, bdonohue@uw.edu
On a Zoom call to discuss study findings, Dr. Chase Cannon was momentarily lost in a memory from 2022. That harrowing summer, an outbreak of mpox, the infection caused by the monkeypox virus, drew hundreds of panicked Washingtonians to the King County Sexual Health Clinic at Harborview Medical Center in Seattle.
“It was crazy,” he said. “We had people lining up around the block at six in the morning. We were in emergency-response mode. Everybody was freaked out, anxious because no one knew what this disease was. Those three months are sort of a blur now.”

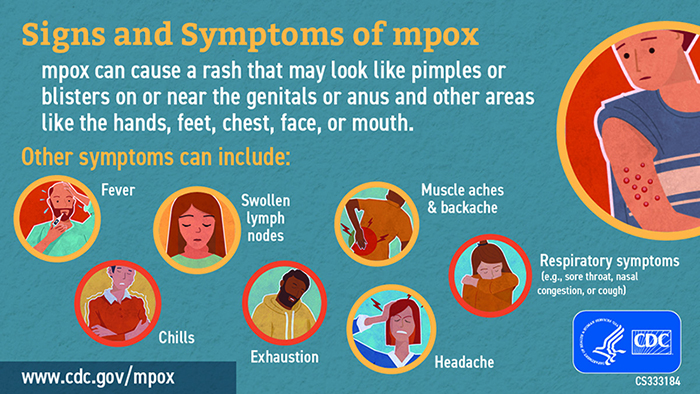
Mpox symptoms include a skin rash lasting upward of one month, fever, muscle aches, fatigue and swollen lymph nodes. Most cases have been reported among men who have sex with men, but women and children have also been infected. Anyone can get mpox — typically from touch, kissing and sex, and less often from contaminated materials such as needles.
Early on, the dearth of reliable public information about the virus and its transmission created worry and urgency among people who wanted to know if they were infected, and if so, what to expect.
The clinic’s providers who saw this influx of patients and noted their symptoms became adept at identifying who actually had mpox. More important, those patients could immediately be offered a prescription of tecovirimat, the only drug available, because it often took five days or more to get lab test results back to confirm the infection.
That is the focus of a paper by Cannon and colleagues, published this month in the journal Sexually Transmitted Diseases. The authors represent UW Medicine and Public Health-Seattle & King County.
Study findings showed that, based on based on talking with and examining the patients, the clinic’s providers accurately predicted and provided same-day tecovirimat to 71% of 121 people whose mpox was confirmed by the gold-standard PCR (polymerase chain reaction) lab test. Clinicians also predicted, with 99% accuracy, which patients would be found mpox-negative by a PCR test.
Cannon acknowledged the World Health Organization’s stance that only a PCR test can definitively confer an mpox diagnosis. But he also described the immense value of a same-day provisional diagnosis.
“In cases where you might send off a swab to get tested and you don’t get the answer back for six days, that’s six days that someone is at home on pins and needles, worried and wondering: Can I see friends? Can I go to work? What if staying home means not getting a paycheck?” he said.
“It’s hugely helpful to tell someone upfront, ‘This really looks like mpox. We’ll send the swab for confirmation, but I’m fairly certain that’s what this is.’ We can start counseling patients and setting their expectations for what will happen, isolation recommendations, how to keep themselves and others safe.”
Getting a same-day prescription is not only a convenience for people who would be challenged to return to the clinic another day, but it also can speed recoveries and protect immunocompromised patients from greater harm, Cannon said.
“We have emerging data that, for people with advanced HIV whose immune systems are more depleted, it’s better to start antiviral treatment sooner. There appears to be a window where, if you wait too long, treatment benefit wanes and patients can progress to more severe cases in that time.”
Although observational data has indicated that tecovirimat shortens the course of mpox, the drug remains investigational because the drug’s safety and effectiveness for treating mpox has not yet been formally established, according to the Centers for Disease Control and Prevention.
That’s why, starting in September 2022, Cannon’s team began inviting patients with PCR-confirmed or presumptive mpox to enroll in a new national study of tecovirimat.
“We know that starting people on treatment before molecular (PCR) test results confirm is not a strategy that has been formally endorsed. But for populations at risk to progress to severe disease, you want to get the ball rolling sooner on treatment, whether we’re prescribing it directly or enrolling them in the trial,” he said.
The outbreak ebbed in the United States and clinicians can now offer at-risk people an mpox vaccine. In Southeast Asia and Africa nations, however, mpox cases are escalating again, this time with a more contagious variant, Cannon said.
For details about UW Medicine, please see our About page.