Vision loss, high cholesterol linked to higher dementia risk
Q&A: Dr. Eric Larson, a coauthor of The Lancet report, talks about ‘modifiable’ risk and the panel’s decision-making process.Media Contact: Brian Donohue - 206-543-7856, bdonohue@uw.edu

A high-profile report today identifies vision loss and high cholesterol as health conditions that can heighten risk of developing dementia. These two additions bring to 14 the number of conditions identified as “potentially modifiable” risks by The Lancet Commission on dementia prevention, intervention and care.

Nearly half of dementia cases could potentially be prevented or delayed by “tackling” these 14 risk factors, the authors surmised.
Previously identified risks include lower levels of education, hearing impairment, high blood pressure, smoking, obesity, depression, physical activity, diabetes, excessive alcohol consumption, traumatic brain injury, air pollution and social isolation.
Among the commission’s 27 members is Dr. Eric Larson, a pioneer of dementia research. He co-founded and was longtime director of the Adult Changes in Thought Study, a joint project of Kaiser Permanente Washington Health Research Institute and the University of Washington, where he is now an affiliate professor in the School of Medicine.
Larson spoke about the commission’s process and his takeaways from the new report — the body’s third such publication since 2017. The Q&A has been edited for length and clarity.
Q: What’s the commission’s big-picture goal with these reports? Are you simply declaring there’s enough evidence about Condition X to make it a risk factor?
Larson: It’s bigger. The thing that gets a lot of attention is the prospect and ideas that dementia can be prevented or have its onset delayed. We’re looking at the evidence as it relates to each domain: prevention, intervention, including drug treatments, and how you provide the best care for people who have dementia.
There appear to be factors that, if modified, the evidence suggests you have a lower risk of developing dementia, at both the public-health level and as an individual, especially in later life.
There’s been an amazing amount of work done since the commission was convened almost 10 years ago. These days there may be 10 or 20 worthy publications (scientific studies) on a single topic from around the world. The money that’s gone into research, especially in the U.S., is striking. It's been very gratifying for me as a graybeard in this area.
Q: What would you highlight from the current report?
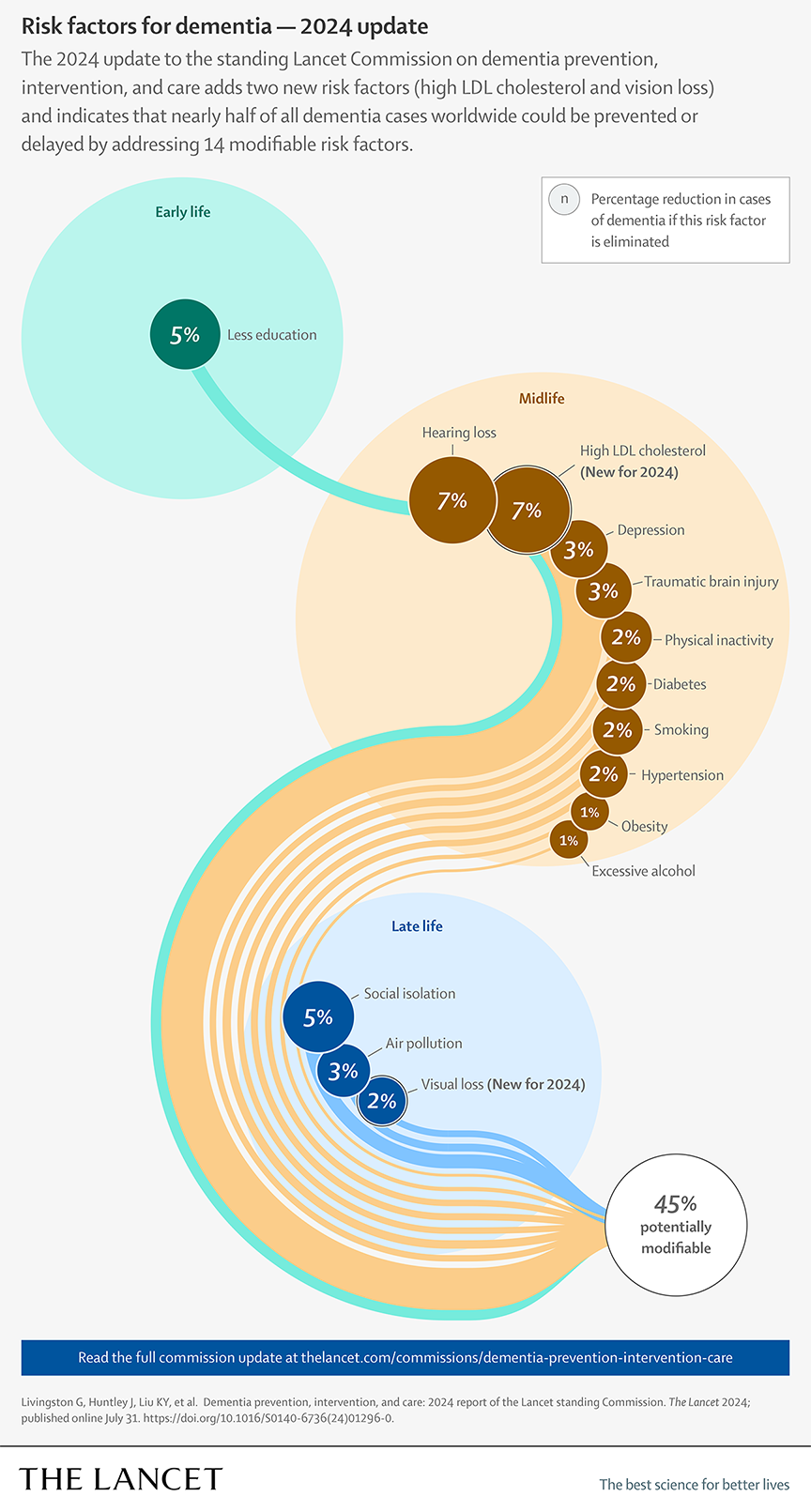
Larson: We estimate that high LDL cholesterol in midlife could add about 7% to someone’s risk for dementia, and that untreated vision loss adds 2% risk. If you take those in isolation, maybe it doesn’t sound important. But when you add up all these risk factors (see graphic) that generally align with overall health, it’s part of a whole cascade of risk. The fact that 45% is theoretically modifiable says something about how we can improve our health and cognitive function in late life. Most of these risk factors also promote general health.
If you look at the midlife risks, a lot of them relate to the health of your blood vessels: cholesterol, physical activity, diabetes, smoking, hypertension, obesity. These are all elements that contribute to the more rapid or earlier onset of damage to the circulatory system.
And in the last couple reports, the thing that has leapt to the fore is the effect of loss of senses. The vision-loss data came from a UW study where Cecilia Lee and her team found that people who have a cataract and get surgery to fix it have a lower rate of dementia compared with people who don’t get it fixed.
So vision appears to be another piece of the puzzle that goes with hearing loss (a previously identified risk). It’s also possible that one of the earliest markers of dementia is loss of smell; years ago, a study of Japanese Americans in King County (the Kame Project) showed that.
All of these sensory inputs to the brain seem important — and balance, too. So, as much as possible, people should protect their senses and correct impaired senses as they age.
Q: How do commission members work? Is there debate about whether there’s enough evidence for a health condition to be formally called out as a risk?
Larson: The topics are teed up in advance of meeting. A team led by University College of London and members of the commission collect papers, and then we gather to discuss the most convincing and important evidence. A group of us drafts individual sections and there is polite conversation among people who have differing views about whether a topic should be approved or not or needs to be modified.
Ultimately the judgment to include a topic is based on the strength and generalizability of the research. The Lancet’s editors work with commission members and especially the leader, Professor Gill Livingston, for revisions in response to independent reviewers and eventual final acceptance in accordance with the journal's peer-review process.
Ultimately, yes, there are items for which the evidence is insufficient to justify inclusion. Sleep and insomnia are an example: How much sleep do you need to nourish your brain? To date, we don’t think the evidence is strong enough to draw a definitive conclusion and recommendation.
Q: How would you characterize these reports’ benefit to patient care?
Larson: I think they are having an effect, but it may be incremental. When I first started in this area, there was very contentious debate about whether exercise helps improve brain function. The generation before me was less keen on exercising.
Now these reports have become part of the health recommendations people get from their doctors and friends and from news stories. Somebody might find out they have high cholesterol and not be too concerned to change their behavior, but when they hear that it’s bad for blood vessels and the brain, maybe they’re motivated by that. Dementia is one of the most dreaded conditions associated with old age.

For details about UW Medicine, please see our About page.